KOM - Atopic Dermatitis Knowledge Challenge: An Educational Symposium
KOM Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterised by intense pruritus and typical skin lesions that has a significant impact on both patients and their families. It can affect daily activities and work productivity1 and accounts for a significant portion of the global burden generated by skin disease.2 AD also has a significant effect on mental health, with almost 25% of patients reporting anxiety as a symptom.3
The pathophysiology of AD is complex and multifactorial. Type 2 immune mechanisms have been recognised as central to pathophysiology, although various immune pathways play a role in the disease. A deeper understanding of these pathways can facilitate the development of targeted therapeutic strategies.4 Blocking interleukin (IL)-4 and IL-13 signalling has a considerable positive effect on skin microbiome and barrier function in AD, with reductions in both the abundance and bioactivity of Staphylococcus aureus in lesional skin.5 Consequently, restoration of skin barrier function is associated with improvements in signs, symptoms and quality of life.6
Dupilumab is a fully human monoclonal antibody that inhibits signalling of IL-4 and IL-13 by targeting the IL-4Rα subunit. By blocking the receptors of IL-4 and IL-13, dupilumab prevents both cytokines from functioning and relieves disease symptoms.7 It is indicated for moderate-to-severe AD in adults and adolescents aged > 12 years and for severe AD in children aged 6–11 years who are candidates for systemic therapy. It can be prescribed with or without topical corticosteroids.8
The Atopic Dermatitis Knowledge Challenge, sponsored by Sanofi and Regeneron Pharmaceuticals, was a highlight of the 2022 meeting of the European Academy of Dermatology and Venereology, held in Ljubljana, Slovenia. Based on an interesting and entertaining quiz format, two experts in the field, Dr Ignasi Figueras and Dr Chih-ho Hong, discussed the pathophysiology of AD and the impact of blocking IL-4 and IL-13 signalling on bacterial colonisation of the skin of patients with AD and on skin barrier function. They also presented the latest real-world evidence on the impact of inadequately controlled disease and addressed long-term control of moderate-to-severe disease.
The burden of moderate-to- severe atopic dermatitis
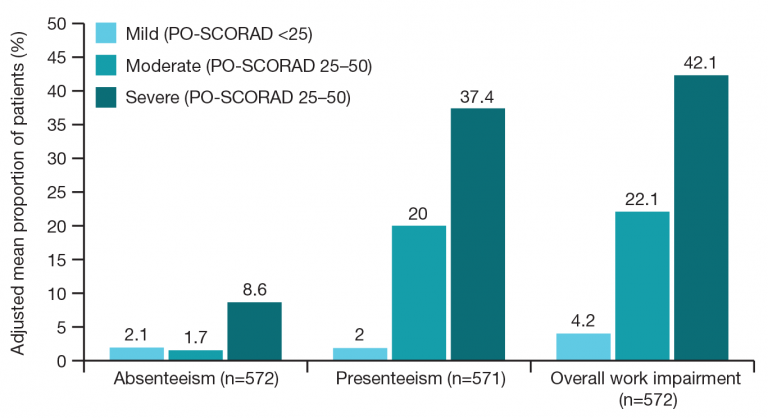
Dr Chih-ho Hong (St Paul’s Hospital, Vancouver, Canada) addressed the effect that moderate-to-severe AD has on patients’ personal and working lives. Over one-third (38%) of patients with moderate-to-severe AD report that their disease has caused them to abstain from a specific career choice.9 AD also has a significant impact on work and work productivity. In an internet-based survey of adults with AD from the population-based National Health and Wellness Survey (Europe 2016, USA 2015 and 2016; n=1232),1 patients were studied by severity (SCORing Atopic Dermatitis [SCORAD] mild, moderate and severe), and those with severe disease were found to be impacted in multiple spheres of their work, mainly in terms of absenteeism and presenteeism (reduced performance in the workplace), and in how they perceived their ability to do their job well (>40%) (Figure 1).
AD is generally known as the ‘itch that rashes’, and its signs and symptoms are associated with a substantial disease burden,10,11 mainly skin lesions, itch and pain, which lead to sleep disruption. Alterations in sleep pattern affect not only patients themselves, but also their partners and family members. Dr Hong stressed the need for clinicians to make every effort to address the impact of sleep disruption on the entire family.
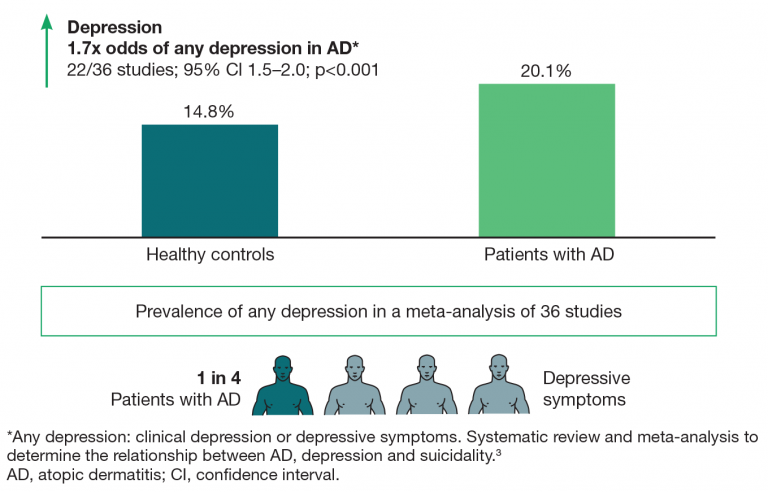
The encompassing nature of AD means that it has a significant impact on mental health. Data from a meta-analysis of 36 studies indicate that depression is 1.7 times more common in patients with AD than in healthy controls, and that almost 1 in 4 patients report anxiety as a symptom (Figure 2).3 More concerning is the finding that suicidal ideation is twice as likely than in healthy controls and that 1 in 8 patients with AD have experienced suicidal ideation at some point in the course of their disease. Dr Hong’s own professional experience has revealed patients whose suicidal ideation was only identified through their participation in AD studies and who required emergency mental health support.
The Atopic Dermatitis in America survey used several measures (Dermatology Life Quality Index [DLQI], Hospital Anxiety and Depression Scale [HADS-A and HADS-D]) to assess AD and quality of life. It found that the impact of AD on quality of life and mental health increases with the severity of AD symptoms.12 Severe disease according to the DLQI (11.4 on a score of 0–30, with 11–20 considered a large effect)13 has a marked impact not only on quality of life, but also on anxiety and depression, and patients with more severe disease are more commonly affected by anxiety and depression, as assessed using the HADS-A and HADS-D scores (10.5 and 8.1, respectively, with 8–10 considered borderline abnormal).14
Skin infection is prevalent in patients with AD and has major consequences for the utilisation of healthcare resources. In a cross-sectional study of almost 5 million patients with AD, identified from the Medical Expenditure Panel Surveys over 20 years, 16% (>750,000) were found to have experienced skin infections.15 When patients with AD are analysed according to whether they have or do not have skin infection, those with skin infection are more likely to use healthcare resources in the form of ambulatory visits (primary care and outpatient dermatology) (p=0.0012), emergency department visits (p=0.0126) and hospitalisation (p=0.0099). In addition, not only do affected patients use more resources, but these resources are also more costly. Again, patients with AD with skin infection incurred significantly greater spending than those without skin infection.15 Dr Hong gave an example from his own experience of a patient with full-body AD who was admitted to the cardiology department after developing sepsis and bacteraemia because of his skin infection. He subsequently developed endocarditis, which required valve replacement, thus dramatically increasing utilisation of healthcare resources and costs.
Patients with AD develop skin infections for various reasons.16 In many cases, the patient has an inherent barrier defect, as measured by transepidermal water loss (TEWL). In addition, the cutaneous microbiome may be altered (dysbiosis), thus leading to a deficiency in commensal bacteria, facilitating the virulence of S. aureus in lesional skin, and enabling this microorganism to colonise the skin. Up to 90% of patients are colonised with S. aureus, which can produce cytotoxins that further damage the skin barrier and enhance immune dysregulation. The resulting skewed immune responses impact cutaneous immunity, predisposing patients to infection.
The pathophysiology of AD
Dr Ignasi Figueras (Bellvitge Hospital, University of Barcelona, Barcelona, Spain) began his presentation by explaining the three major types of cell-mediated immunity underlying the pathophysiology of AD, namely, type 1, type 2 and type 3, each of which has a specific inflammatory pathway.4,17-22 The type 1 pathway is mediated mainly by macrophages, NK cells, and Th1 cells; its primary targets are intracellular bacteria and viruses. The type 2 pathway is mediated by Th2, ILC2 and mast cells, with its main targets being helminths and other parasites. Finally, the type 3 pathway is mediated principally by neutrophils, but also by innate lymphoid cells (ILCs) and Th17 and Th22. Its main targets are extracellular bacteria and fungi.
Dysregulation of the type 2 pathway leads to type 2 inflammatory diseases, including AD.
Type 2 inflammation is both local and systemic and may involve various organs and systems.23-28 For example, ear, nose and throat involvement can take the form of chronic rhinosinusitis and allergic rhinitis. This type of inflammation leads to asthma and eosinophilic chronic obstructive pulmonary disease when present in the lungs and to eosinophilic esophagitis when present in the gastrointestinal tract. As for the skin, type 2 inflammation has also been associated with prurigo nodularis, bullous pemphigoid and chronic spontaneous urticaria, in addition to AD.
IL-4 and IL-13 are both key (i.e. critical) drivers and central (i.e. dominant) drivers in type 2 inflammation.2,23,30-32 Their importance arises from their mediation in the pathophysiologic consequences of type 2 inflammation in disease and the subsequent signs and symptoms induced. As mediators, IL-4 and Il-13 exert effects at various levels. They are involved in barrier dysfunction and tissue remodelling,2,23,30-31 neuroimmune dysfunction (e.g. itch, smell, cough, dysphagia),2,30-32 smooth muscle contractility,23 microbiome alterations2,30 and mucus production.23,30 IL-4, in particular, plays a key role in production of IgE and in trafficking of inflammatory cells to tissues.2,23,30,31
Dr Figueras highlighted the role of type 2 inflammatory cytokines, including IL-4 and IL-13, as a link between the skin barrier, immune activation and itch.23,33-36 External allergens and antigens can penetrate the epidermis, where they are taken up by Langerhans cells. These then migrate to the lymph nodes, where, under the effect of alarmins (e.g. thymic stromal lymphopoietin [TSLP], IL-33 and IL-25), the inflammatory response switches from a Th0 to a Th2 response. IL-4 is a key cytokine in this process. The lymphocytes migrate back to the bloodstream and then to the dermis, where they produce IL-4 and IL-13, worsening barrier disruption and contributing to itch. Therefore, by blocking both these cytokines, itch can be blocked.
Alterations in the skin microbiome can also play a role in driving type 2 inflammation and skin barrier dysfunction in AD. Overgrowth of S. aureus leads to more pronounced colonisation in the skin of patients with AD compared with healthy individuals.37,38 Therefore, alteration of the microbiome is not only a consequence, but also a cause of AD. Colonisation by S. aureus can induce type 2 inflammation, host cytotoxicity, mast cell activation, IgE production, keratinocyte alarmin production (TSLP, IL-25 and IL-33), and, epidermal barrier disruption.37,39-41
The impact of blocking IL-4 and IL-13 signalling on skin microbiome and barrier function in AD

Dr Hong reviewed data presented in poster format at the 2022 annual meeting of the American Academy of Allergy, Asthma and Immunology by Beck et al.5 The data show that dupilumab is associated with dramatic reductions in S. aureus culture in the skin of patients with AD. Traditionally, skin infections were treated with antibiotics and bleach baths, and clinicians were unaware that targeted treatment can actually alter the microbiome.
In the ADRN09 study,5 a multi-centre, randomised, double-blind placebo-controlled trial, dupilumab was administered for 6 weeks. The authors quantified S. aureus and analysed barrier function. S. aureus was recovered by culture from lesional and non-lesional skin. In the dupilumab-treated group, the culture count (colony-forming unit [CFU]/cm2) decreased dramatically from as early as 3 days, not only in lesional skin, but also in non-lesional skin. The same effect is observed irrespective of whether the skin is assessed using culture or more sensitive approaches such as quantitative polymerase chain reaction (PCR) assay. The results are even more dramatic after 14 days.
In addition to culture and quantitative PCR, analysis of the cytotoxins produced by S. aureus shows that cytotoxin activity related to S. aureus is also reduced only by using dupilumab as treatment. These reductions in bioactivity are seen at ≥7 days in lesional skin, although they take slightly longer in non-lesional skin (≥21 days). Therefore, treatment with dupilumab leads to significant improvements in infection.
Dr Hong presented further data from the ADRN09 study to support the effects of dupilumab on skin barrier function. The study was based on the analysis of TEWL, a surrogate marker of skin barrier function, which measures how much water is leaving the skin into the external environment. Improvements in TEWL suggest that the skin barrier is being repaired. In the study, Beck et al5 only gave the patients dupilumab, finding that dupilumab alone improved skin barrier function. The improvement in TEWL was already statistically significant at day 3 (p=0.02), although this was more apparent at day 42 (p=0.03).
In another exploratory study performed by Bissonnette et al6, BALISTAD, the authors assessed the use of dupilumab on barrier function and the lipid characteristics of the skin barrier. The authors found that dupilumab restored skin barrier function and that this was associated with an improvement in signs, symptoms and quality of life in the patient with AD. Photographic evidence revealed a clear improvement in skin lesions after 16 weeks (Figure 3).
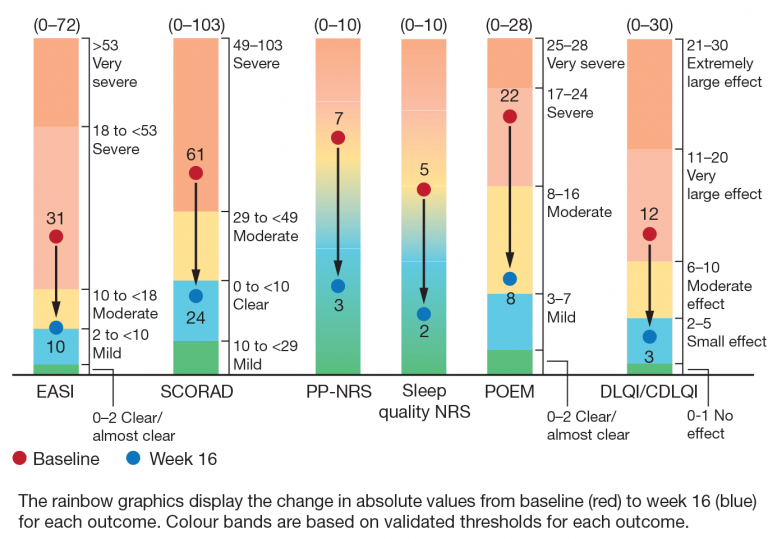
The authors analysed the patients’ progress over 16 weeks using a series of instruments and reported the improvement in absolute values from baseline to week 16 for each outcome. The Eczema Area and Severity Index (EASI) score fell from 31 to 10 (0–72), and SCORAD from 61 to 24 (0–103). Improvements were also recorded for itch (Peak Pruritus Numerical Rating Scale [PP-NRS] from 7 to 3 [0–10]), sleep (Sleep Quality NRS, 5 to 2 [0–10]), eczema (Patient Oriented Eczema Measure [POEM], 22 to 8 [0–28]), and quality of life (DLQI, 12 to 3 [0–30]) (Figure 4). Therefore, the authors reported not only a clinical improvement, but also an improvement in objective metrics commonly used to assess atopic dermatitis.
Real-world considerations for long-term systemic therapy of AD
Dr Figueras explained that there are unmet needs when using conventional systemic therapies for the long-term management of moderate-to-severe AD. Very often, the length of treatment with systemic immunosuppressants is limited by adverse effects and the possibility of disease flare with withdrawal. In addition, patients may experience intensified disease activity for 30%–50% of the year. Historical treatment paradigms, which are based on oral corticosteroids and immunosuppressants, primarily address disease manifestations using a reactive, episodic approach.42-44
When considering the long-term approach to AD, it is important to consider how data from studies translate into the real-world setting. Dr Figueras highlighted the wealth of published real-world experience in AD (some 76 published studies), showing that dupilumab is approved for the treatment of adults with moderate-to-severe AD in 60 countries. Published real-world studies provide data on a total of 12,189 patients with AD from 30 countries, thus supporting the effectiveness and safety of dupilumab in routine clinical practice.
AD is a chronic, lifelong disease for which a rapid and sustained response is needed. The response should take into account severity, quality of life and itch. Of particular interest, data on treatment with dupilumab reported from the Netherlands and Japan by de Wijs et al45 show that a fast response is achieved in terms of EASI and that this is maintained over time (18 months). Similar findings can be seen with the PP-NRS and DLQI instruments.
Infection is a common problem in patients with AD. In their retrospective observational study, using data from the US Optum Clinformatics® database and presented at the Annual Meeting of the American Academy of Dermatology (AAD 2022), Ong et al46 found that dupilumab significantly reduced the prevalence of skin infections — bacterial, fungal and viral — in the real-world setting after 12 months (from 24.7% to 11.2%). In addition, the use of systemic and topical antibiotics and antifungals was also significantly reduced after initiation of dupilumab.
Dupilumab has been shown to be safe for treatment of moderate-to-severe AD in the long term. Dr Figueras presented data from Beck et al,47 who found that adverse events were similar at 4 years, the most frequent being nasopharyngitis, upper respiratory tract infection and conjunctivitis, at both 52 and 104 weeks. Of note, rates of total herpesvirus infections, eczema herpeticum and herpes zoster were numerically lower in the open-label extension study than with placebo plus topical corticosteroids (6.78 vs. 9.17; 0.23 vs. 2.13; 0.97 vs. 1.77).
What are the most important considerations when selecting a long-term systemic therapy for patients with AD?
In the panel discussion, both speakers agreed that when addressing the patient with AD, it is of the utmost importance to stress that their disease is chronic and that it must be managed using chronic disease strategies. Patients are often frustrated by their disease: flare-ups are common, and it is often necessary to visit a primary care physician and even the emergency department, where they are prescribed corticosteroids, only to experience subsequent flare-ups. However, to some extent, patients are aware of their problem and of the fact that they need therapy that will provide them with better control in the long term (fewer flare-ups, fewer visits to the emergency department and improved quality of life).
Talking to the patient requires the physician to think in terms of the art of medicine, as opposed to the science of medicine, translating the results of research into clear, tangible advantages for the management of AD. When talking to the patient, the physician should try to frame treatment in terms that the patient can understand with respect to activities of daily living. For example, patients should be informed that they can go swimming, participate in sports and do their jobs fully again, because they are receiving treatment that completely controls disease. Dr Hong quoted the example of a 20-year-old woman who experienced skin infection related to eczema once a month, with lymphoedema in her legs because of repeated infections. She visited the emergency department regularly, was prescribed antibiotics and was hospitalised twice a year. Since starting dupilumab, she has not had to go to hospital once. Using this anecdote with other patients enables them to see reflections of their own situation and how their quality of life can improve through the realistic benefits of treatment (e.g. being able to wear dark clothing, participate in sports). Often, once the patient sees the advantages dupilumab can bring, they overcome their reservations and take on a positive attitude towards the long-term management of their disease.
When talking about the risks of treatment, according to Dr Figueras, the approach to be taken is that of enabling the patient to balance the risks against the benefits and to stress that dupilumab has a good safety profile. In any case, patients’ frustration with their current situation often makes them receptive to any approach that can improve their quality of life. Dr Hong introduced the notion of the ‘side effects of not being treated’. In other words, while it is necessary to inform patients of the side effects of treatment, it is also important to highlight the side effects of not being treated, not only in terms of clothing, leisure activities and employment prospects, but also in terms of the potential for anxiety and depression to develop.
The approaches used in clinical practice when evaluating disease control include various metrics, some of which focus on long-term disease control, such as the Atopic Dermatitis Control Tool (ADCT) and RECAP (Recap of atopic eczema), which can be used both in clinical trials and in clinical practice. While more traditional tools such as EASI and DLQI are valid, they are limited by the fact that they do not provide information on how the disease is being controlled from one timepoint to another. Both the ADCT and RECAP provide additional insight into how well the disease is being managed over time. Outcome measurement instruments are important and provide clinicians with an abundance of information before they see the patient for the first time. However, it is important to remember that the patients being treated are people and not numbers, and that information on the patient’s daily life is equally useful as that provided by instruments and should be considered before deciding on therapy. Consequently, talking to patients directly about their disease is highly revealing.
Therapy with dupilumab can be transformational, enabling patients to lead normal lives. For example, adolescents with AD may have to miss school because of how the disease interferes with daily life, even to the extent that they must repeat full years of study. Dupilumab makes it possible for them to attend school at the same level as their peers.
Conclusions
The continuous disease burden of AD can have a significant and cumulative impact beyond the signs and symptoms of disease, including career choices and mental health. In fact, the impact on quality of life and mental health, in particular, increases with the severity of symptoms.
The pathophysiology of AD is driven by underlying systemic type 2 inflammation, with IL-4 and IL-13 as key and central type 2 cytokines in pathogenesis. Both cytokines mediate effects on the immune response, barrier dysfunction, itch and the skin microbiome.
Therapy with dupilumab led to rapid improvements in S. aureus counts and skin barrier function. The abundance of this microorganism was rapidly reduced, as was the bioactivity of its cytotoxins. This reduction correlated with improvements in disease activity as measured by SCORAD. Dupilumab also led to significant improvements in skin barrier function, as reflected in improvements in clinical signs, symptoms and quality of life in patients with AD.
The long-term effectiveness of dupilumab is supported by data not only from clinical trials, but also from relevant real-world studies worldwide. Patient testimony of the life-changing effects of treatment can help when educating untreated patients about the benefits of dupilumab.
References
- Andersen L, Nyeland ME, Nyberg F. Increasing severity of atopic dermatitis is associated with a negative impact on work productivity among adults with atopic dermatitis in France, Germany, the UK and the USA. Br J Dermatol. 2020; 182(4): 1007–1016.
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020; 396: 345–360.
- Patel KR, Immaneni S, Singam V, Rastogi S, Silverberg JI. Association between atopic dermatitis, depression, and suicidal ideation: a systemic review and meta-analysis. J Am Acad Dermatol. 2019; 80(2): 402–410.
- Eyerich K, Eyerich S. Immune response patterns in non-communicable inflammatory skin diseases. J Eur Acad Dermatol Venereol. 2018; 32(5): 692–703.
- Beck L. Poster presented at: #AAAAI22 annual meeting. February 25–28, 2022, Phoenix, AZ, USA. S2521.
- Bissonnette R, Leung DYM, Bologna G, Levit NA, Rossi AB, Zhang A. Dupilumab treatment restores skin barrier function and improves clinical and patient reported outcomes in adults and adolescents with moderate to severe atopic dermatitis. Poster presented at the 2022 Annual Meeting of the American Academy of Dermatology, March 2022.
- European Medicines Agency. Dupixent. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/dupixent. Accessed May 2022.
- Sanofi. Dupixent (Dupilumab) Abbreviated Prescribing Information 300 mg. Available
at https://www.campus.sanofi/dam/
jcr:f93de307-05a4-45fa-8732-a939b4c19eca/Dupixent.pdf. Accessed May 2022. - Holm EA, Esmann S, Jemec GBE. The handicap caused by atopic dermatitis—sick leave and job avoidance. J Eur Acad Dermatol Venereol. 2006; 20(3): 255–259.
- Simpson EL, Bieber T, Eckert L, Wu R, Ardeleanu M, Graham NMH, Pirozzi G, Mastey V. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol. 2016; 74(3): 491–498.
- von Kobyletzki LB, Thomas KS, Schmitt J, Chalmers JR, Deckert S, Aoki V, Weisshaar E, Ojo JA, Svensson Å. What factors are important to patients when assessing treatment response: an international cross-sectional survey. Acta Derm Venereol. 2017: 97(1): 86–90.
- Chiesa-Fuxench ZC, Block JK, Boguniewicz M, et al. Atopic Dermatitis in America Study: a cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol. 2019; 139(3): 583–590.
- Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science
of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol. 2005; 125(4): 659–664. - HADS. Available at: http://www.svri.org/sites/default/files/attachments/2016-01-13/HADS. pdf. Accessed May 2022.
- Sandhu JK, Salame N, Ehsani-Chimeh N, Armstrong AW. Economic burden of cutaneous infections in children and adults with atopic dermatitis. Pediatr Dermatol. 2019; 36(3): 303–310.
- Wang V, Boguniewicz J, Boguniewicz M, Ong P. The infectious complications of atopic dermatitis. Ann Allergy Asthma Immunol. 2021; 126(1): 3–12.
- Kaiko GE, Horvat JC, Beagley KW, Hansbro PM. Immunological decision-making: how does the immune system decide to mount a helper T-cell response? Immunology. 2008; 123(3): 326–338.
- Raphael I, Nalawade S, Eagar TN, Forsthuber TG. T cell subsets and their signature cytokines in autoimmune and inflammatory diseases. Cytokine. 2015; 74(1): 5–17.
- Nakayama T, Hirahara K, Onodera A, Endo Y, Hosokawa H, Shinoda K, Tumes DJ, Okamoto Y. Th2 cells in health and disease. Annu Rev Immunol. 2017; 35: 53–84.
- Coates LC, FitzGerald O, Helliwell PS, Paul C. Psoriasis, psoriatic arthritis, and rheumatoid arthritis: is all inflammation the same? Semin Arthritis Rheum. 2016; 46(3): 291–304.
- Gandhi NA, Pirozzi G, Graham NMH. Commonality of the IL-4/IL-13 pathway in atopic diseases. Expert Rev Clin Immunol. 2017; 13(5): 425–437.
- Artis D, Spits H. The biology of innate lymphoid cells. Nature. 2015; 517(7534): 293–301.
- Gandhi NA, Bennett BL, Graham NM, Pirozzi G, Stahl N, Yancopoulos GD. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016; 15(1): 35–50.
- Carr S, Watson W. Eosinophilic esophagitis. Allergy Asthma Clin Immunol. 2011; 7 Suppl1(Suppl 1): S8.
- Steinke JW, Wilson JM. Aspirin-exacerbated respiratory disease: pathophysiological insights and clinical advances. J Asthma Allergy. 2016; 9: 37–43.
- Maurer M, Altrichter S, Schmetzer O, Scheffel J, Church MK, Metz M. Immunoglobulin
E- mediated autoimmunity. Front Immunol. 2018; 9: 689. - Iking A, Grundmann S, Chatzigeorgakidis E, Phan NQ, Klein D, Ständer S. Prurigo as a symptom of atopic and non-atopic diseases: aetiological survey in a consecutive cohort of 108 patients. J Eur Acad Dermatol Venereol. 2013; 27(5): 550–557.
- Lee GR, Maarouf M, Hendricks AK, Lee DE, Shi VY. Current and emerging therapies for hand eczema. Dermatol Ther. 2019; 32(3): e12840.
- Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018; 4(1): 1.
- Schleimer RP. Immunopathogenesis of chronic rhinosinusitis and nasal polyposis. Annu Rev Pathol. 2017; 12: 331–357.
- Davis BP, Rothenberg ME. Mechanisms of disease of eosinophilic esophagitis. Annu Rev Pathol. 2016; 11: 365–393.
- Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf. Updated 2021. Accessed May 2022.
- Noda S, Krueger JG, Guttman-Yassky E. The translational revolution and use of biologics in patients with inflammatory skin diseases. J Allergy Clin Immunol. 2015; 135: 324–336.
- Wynn TA. Type 2 cytokines: mechanisms and therapeutic strategies. Nat Rev Immunol. 2015; 15: 271–282.
- Stott B, Lavender P, Lehmann S, Pennino D, Durham S, Schmidt-Weber CB. Human IL-31 is induced by IL-4 and promotes TH2-driven inflammation. J Allergy Clin Immunol. 2013; 132: 446–454. E5.
- Kong DH, Kim YK, Kim MR, Jang JH, Lee S. Emerging roles of vascular cell adhesion molecule-1 (VCAM-1) in immunological disorders and cancer. Int J Mol Sci. 2018; 19(4): 1057.
- Li W, Yosipovitch G. The role of the microbiome and microbiome-derived metabolites in atopic dermatitis and non-histaminergic itch. Am J Clin Dermatol. 2020; 21(Suppl 1): 44–50.
- Bjerre RD, Bandier J, Skov L, Engstrand L, Johansen JD. The role of the skin microbiome in atopic dermatitis: a systematic review. Br J Dermatol. 2017; 177(5): 1272–1278.
- Kim J, Kim BE, Ahn K, Leung DYM. Interactions between atopic dermatitis and Staphylococcus aureus infection: clinical implications. Allergy Asthma Immunol Res. 2019; 11(5): 593–603.
- Paller AS, Kong HH, Seed P, Naik S, Scharschmidt TC, Gallo RL, Luger T, Irvine AD. The microbiome in patients with atopic dermatitis. J Allergy Clin Immunol. 2019; 143(1): 26–35.
- Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016; 387(10023): 1109–1122.
- Zuberbier T, Orlow SJ, Paller AS, Taïeb A, Allen R, Hernanz-Hermosa JM, Ocampo-Candiani J, Cox M, Langeraar J, Simon JC. Patient perspectives on the management
of atopic dermatitis. J Allergy Clin Immunol. 2006; 118: 226–232. - Leung DYM, Boguniewicz M, Howell MD, Nomura I, Hamid QA. New insights into atopic dermatitis. J Clin Invest. 2004; 113: 651–657.
- Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018; 32(6): 850–878.
- De Wijs LEM, Fujimoto RFT, Andrinopoulou ER, Nijsten T, Hijnen D, Kataoka Y. Dupilumab treatment in patients with atopic dermatitis: a comparative cohort study between the Netherlands and Japan shows a discrepancy in patient-reported outcome measures. Br J Dermatol. 2021; 185: 555–562.
- Ong P, Cork MJ, Armstrong A, Wollenberg A, Zhang A, Lubwama R. Real-world analysis of skin infections and antimicrobial use among patients with atopic dermatitis before and after initiation of dupilumab treatment. Poster presented at the 2022 Annual Meeting of the American Academy of Dermatology, March 2022.
- Beck LA, Deleuran M, Bissonnette R, et al. Dupilumab provides acceptable safety and sustained efficacy for up to 4 years in an open-label study of adults with moderate-to-severe atopic dermatitis. Am J Clin Dermatol. 2022; 1–16. doi: 10.1007/s40257-022-00685-0.